COVID-19: end of life care and the lessons of the first wave
Marie Curie-Nursing Standard survey highlights the emotional toll of the pandemic and the need for more staff support
- Survey reveals the impact on nurses who provided end of life care for increased numbers of patients during the first wave
- The need to wear personal protective equipment and the restrictions on families visiting changed the way end of life care was provided
- How nurses can access emotional and mental health support

difficult aspects of the first wave Picture: iStock
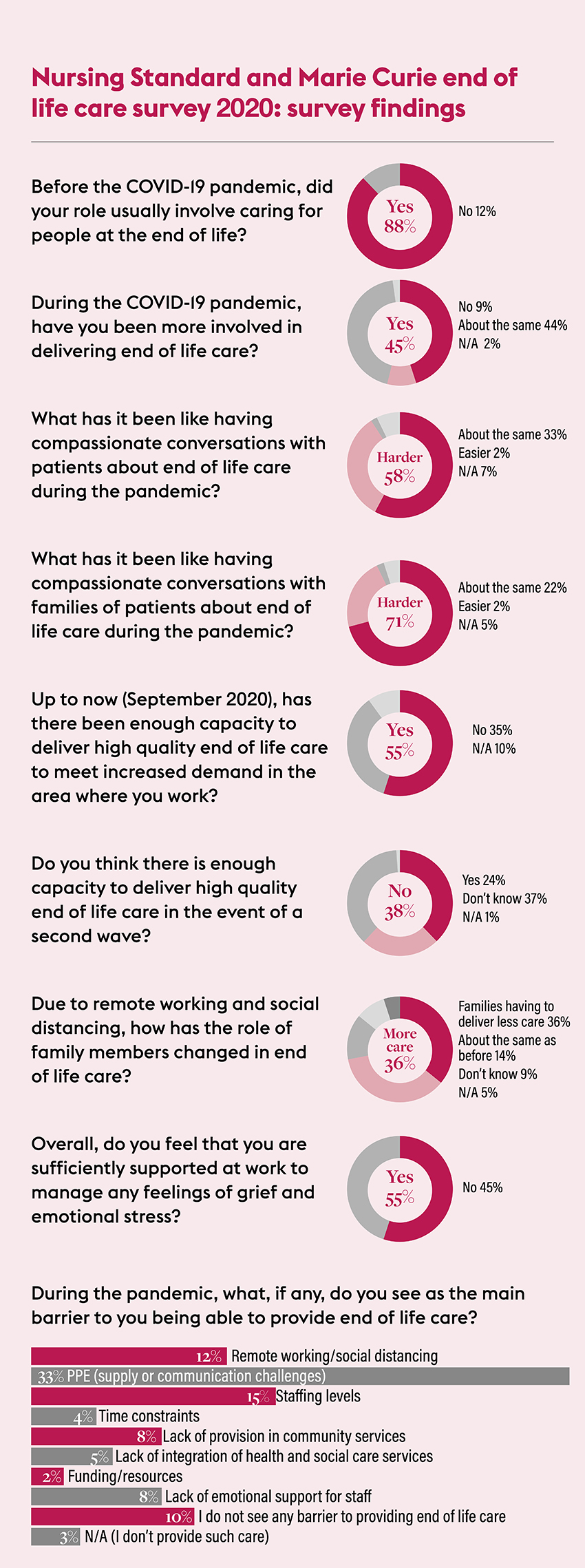
One in three nurses feel they did not have the capacity to provide high quality end of life care as deaths rose during the first wave of the COVID-19 pandemic, a survey by Nursing Standard and end of life charity Marie Curie suggests.
Face masks hampered good communication, while restrictions on families visiting was distressing for patients, relatives and staff, according to respondents to the survey, which was carried out in September.
The emotional impact of providing end of life care in the first wave
Many highlighted the distress of being unable to touch or comfort patients and relatives.
‘The human connection is harder to achieve,’ one nurse told the survey, which received 894 responses.
Another described making a phone call to a relative to tell them a loved one had died as ‘one of the most difficult things I’ve ever had to do’.
‘I put the phone down and cried my heart out,’ the respondent said. ‘To give someone bad news over the phone, not knowing where they are and who they are with, not holding their hand or sitting down with them, was horrible.’
Almost half (45%) of those who responded to our survey said they had undertaken more end of life care than they usually would since the pandemic began in early 2020.
Coping with many more resident and patient deaths than usual
For some, particularly those on acute wards and in care homes, COVID-19 bought many more deaths than usual.
One care home worker said 15 residents at the home where they work had died from the virus. ‘It was so painful losing our residents, we looked after them for many years,’ they wrote.
One nurse said at their workplace three or four patients a day had died from COVID-19 during the first wave, and on one day nine patients died.

placed an emotional burden on staff’
Marie Curie chief nurse and executive director of caring services Julie Pearce said that nurses found providing end of life care physically and emotionally challenging during the first wave of the pandemic.
‘While it is clear from the responses, and from what we hear from our own staff, that everybody did their best in difficult circumstances, there were some standout issues that really affected the quality of end of life experiences,’ she said.
‘Face masks and visors limited communication and nurses were unable to touch and get close to patients and families, and these are a fundamental part of end of life care. This was felt acutely by nurses,’ Ms Pearce says.
End of life care when visitor numbers are limited
‘The other aspect that really came out strongly was visiting. This posed a real dilemma and tension for nurses, the balance between keeping staff and patients safe and the distressing need to limit visiting to one or two family members for a short period of time when a patient was at the end of life.
‘The issues around visiting placed an emotional burden on staff and feelings that they had not been able to meet the real need for patients and their families to be together. Nurses are acutely aware of the impact this is likely to have had on families and their ability to grieve.’
‘A dying person’s last contact with another person is through a gloved hand and a smile not seen because of the mask’
Survey respondent
A third of the respondents (33%) said personal protective equipment (PPE) was the main barrier to providing good end of life care, followed by the impact of social distancing and remote working (12%).
Many told how the physical barrier of PPE made it harder to communicate well and provide comfort as well as touch. It left patients uncertain about who was caring for them and made discussions impersonal.
‘Not being able to physically and emotionally console distressed relatives – a hug or simply taking time to have a cup of tea with them,’ one respondent said when highlighting the difficulties.
Another said: ‘A dying person’s last contact with another person is through a gloved hand and a smile not seen because of the mask.’
Delivering the family’s wishes to the patient
Nurses also reported being with patients during their final hours more than they would have done previously. ‘I am spending more time with patients on end of life as there are limitations on family visits’ one said.
‘Not having the relative with the patients during the time of death felt like a huge responsibility on nursing staff to get it absolutely right,’ another said.
‘To be a companion and deliver the family’s wishes to the patients – during COVID it felt like the nursing staff absorbed the emotions when our patients died.’

Picture: iStock
Others said the ban on visitors meant that dying patients spent more time alone. One said limits on staff time meant ‘patients did not have someone holding their hand and reassuring them at the end’.
Having compassionate conversations about end of life care with patients and families was more difficult during the pandemic, nurses agreed. Almost 60% of respondents felt such discussions were more difficult with patients, and 70% with relatives.
‘Not having the relative with the patients during the time of death felt like a huge responsibility on nursing staff to get it absolutely right’
Survey respondent
In other cases, some said they feared that patients in need of end of life care stayed at home as they wanted to be with their family, or were afraid of contracting COVID-19 if they went into hospital.
This meant relatives carrying out more care at home than they normally would have done, they said, and nurses feared patients had less than optimal control for their symptoms.
‘Fewer patients wanted to be admitted to the hospice as they could not have any visitors,’ one nurse said. ‘We worked alongside the district nurses to support patients at home.’
‘Some deaths I saw are still constantly on my mind’
More than half of the survey respondents (55%) felt they had sufficient support to cope with feelings of grief and emotional stress during the pandemic, while 45% did not.
For many who responded to the survey, the most vital support came from colleagues in close-knit teams. But some said they were struggling with what they had seen and experienced during the first wave of COVID-19.

New methods of support for depleted staff
A number said they or their colleagues were showing signs of post-traumatic stress disorder (PTSD).
‘There is no support proactively offered even to staff showing clear PTSD symptoms,’ one said. ‘Some deaths I saw are still constantly on my mind.’
Social distancing and working remotely had damaged some of the support systems that nurses had in place before the pandemic. ‘Previously nurses met every 6-8 weeks for clinical supervision, which was an excellent support mechanism. We need to meet again, aware of social distancing. It is important to find ways of support,’ one nurse said.
Recognising when to seek support
Those working for specialist charities, such as Marie Curie and Macmillan Cancer Support, suggested they had better support in place than NHS staff.
Many nurses reported employers signposting to apps and remote services. But for some this was insufficient and could not replace face-to-face debriefs and support.
But others said the pandemic had been a time of good mental health support. ‘I have worked in palliative care for over 20 years and feel that I have had the best emotional support ever. I also have been encouraged to develop resilience and to recognise when I need support.’
Where to go for mental health support
Community nursing teams took on extra patients – with extra responsibilities
GPs and some specialist palliative care services stopped face-to-face visits, meaning community nursing teams were trying to care for more patients. ‘We hardly see a GP, meaning we are taking on more complex decisions,’ one nurse said.
Conducting the survey
The Nursing Standard and Marie Curie survey asked nurses to share their experiences of providing end of life care during the COVID-19 pandemic.
The survey was conducted using the Survey Monkey online survey website and was open from 7–28 September 2020.
It was promoted via email to registered users of RCNi.com, on social media and in online news articles.
It received 894 responses and the findings were analysed by Nursing Standard staff.
The speed at which some patients deteriorated with COVID-19 meant that some important discussions around preparation and planning did not take place.
‘Patient demographics changed and we were seeing quicker onset of illness in patients rather than chronic disease, which often meant these conversations could not be had,’ one nurse said.
Staffing pressures ‘unsustainable’
High levels of staff sickness, or staff isolating while waiting for a test or results, combined with existing low staffing levels have exacerbated the difficulties – and continue to do so, the survey heard.
‘Staffing has been appalling,’ one nurse said. ‘There are a number of members of staff with small children and already two are off because their children have had a temperature and the schools have sent them home. This will be unsustainable for the NHS.’
Another said: ‘Everyone with a cold has to be tested in order to be able to work safely. More and more staff are absent with a cold and pressure has increased on the staff at work.’
Patient-centred care was at times difficult in the fast-moving and pressured circumstances created by the pandemic.
It made care ‘less personal for patients and relatives‘, one nurse said: ‘While the physical standards of patient care arguably remained high, the holistic care of the patient and relative was reduced due to visiting restrictions.’
RCN deputy director of nursing Jude Diggins said the survey findings highlight the 'truly heartbreaking circumstances' facing nurses during the pandemic.
'It's not surprising that caring for patients at the end of their life in these unprecedented working conditions is leaving some of them feeling exhuasted or even traumatised.
'NHS, social care and other employers must ensure that staff have time to talk about their experiences, whether that's through formal counselling or conversations with their colleagues.'
How pressures improved some aspects of end of life care
Some nurses told the survey that the pandemic had brought improvements in how they work, including closer working between teams and better use of appropriate remote consultations.

families when they are unable to be
with each other at the end of life
Greater availability of anticipatory medication in patients’ homes, and better coordination between hospice and other care staff should be maintained, respondents said.
The depth of nurses’ feelings for relatives unable to be with dying patients and residents is clear, and this has led to new approaches to help them keep in touch.
Giving knitted hearts to patients at the end of life as well as to their next of kin helped create a sense of contact, a number of respondents said.
‘We have started to provide memory boxes that we make for patients’ families, bereavement books and sympathy cards which we send to tell families who was with their loved ones and who cared for them,’ one nurse said.
‘Prepared for more heartbreak’ amid the second wave
Concerns about end of life care during the second wave of COVID-19 were evident in survey responses.
Almost four in ten (38%) respondents said they do not think there is enough capacity to provide high quality end of life care throughout the second wave.

As cases continue to rise rapidly across the UK and the NHS prepares for the increased demands of this winter season, Marie Curie has raised concerns about how providers of end of life care will cope.
These pressures, combined with the backlog of people who missed out on crucial diagnoses or treatment during lockdown, will see more people than ever needing extra care and support at the end of life, the charity warns.
Too emotionally depleted to cope with another surge
These concerns were echoed in our survey responses.
‘Our staff are prepared for more heartbreak,’ one respondent said.
‘Community services already struggling now,’ another said. ‘A second wave will mean patients and families will not receive high quality end of life care.’
Another added: ‘We are at our limits, caseload keeps increasing with no sign of let up.’
Many respondents said nurses were too emotionally depleted and drained to cope with a second wave.
‘I don’t think nurses have much resilience left,’ one said, ‘We are tired, burned out from absorbing the first phase.’
But some felt that the experience and knowledge gained from the first round would allow services to cope better this time.
‘We are more prepared than before,’ one respondent said. ‘We now have measures in place to prevent the spread of the virus in hospital and we are more organised.’
Erin Dean is a freelance health journalist